This is a trial of NAD+ infusions in patients with many different disease processes. Studies in 2018 and 2021 showed that NAD+ infusion allows cells to have more ATP. NAD+ is one of the rate-limiting factors in the conversion of ADP to ATP. By infusing NAD+, the patient has an increased amount of ATP. The code to repair cells and repair DNA damage, cancer, diabetes, aging, many other disease processes is already in our DNA. By providing additional ATP, the cell is able to regenerate itself. This is the theory behind IV-medical.com.
this is the background information for the clinical trial.
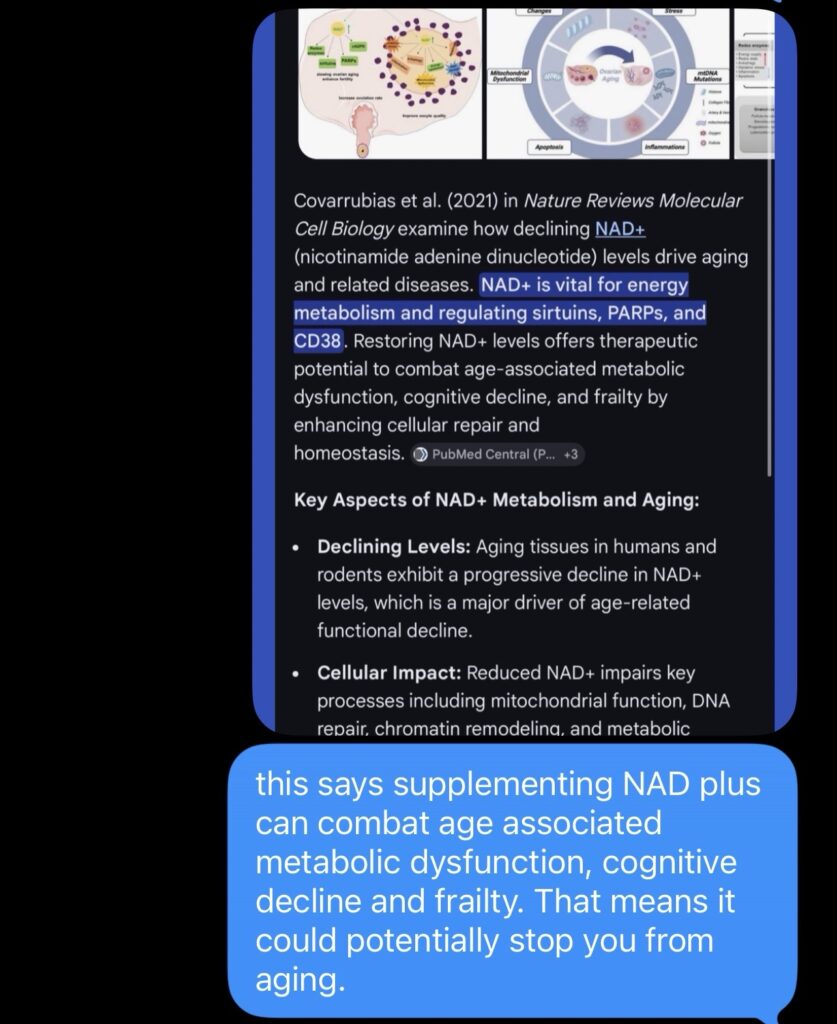
imagine if monthly or weekly NAD plus infusion cured cancer. That’s what these preliminary studies are suggesting. It cures all diseases including aging, dementia, diabetes, obesity. Why hasn’t this been studied? These studies came out in 2018-2021 during the COVID epidemic.
imagine if NAD+ infusions of say 250ml weekly or monthly prevented CHF exacerbations by providing stunned or weakened myocardial and endocardial cells with extra NAD+. perhaps weekly infusions of NAD+ provide extra cellular power to help the cell’s metabolism to regenerate myocardium or endocardoum or purkinje fibers or neurons. the possibilties are endless and should all be studied given how cheap this medication is and how effective it has been shown to be in these preliminary studies. perhaps even ocular tissue could be helped to regenerate. basically my theory is that NAD+ infusions help the body heal and regenerate itself and therefore could be the key to living forever.
kalki bommaraju md mph
1:55 am
3/28/2026
I am proposing an NIH and CDC sponsored clinical trial of NAD plus infusions—weekly or monthly—in all oncologic patients and all patients with diabetes type one or type two and all patients with obesity and all patients with dementia and all patients with Alzheimer’s dementia, and all patients with any signs of aging to see if NAD plus infusions reverse any of these processes.
The cost of an NAD plus IV infusion is about $10 plus whatever the cost of NAD plus is which I’m sure is minimal. There is no reason not to do this study other than no one can really profit from this other than IV-MEDICAL.COM and other cool doctors like Philip F Binkley MD MPH CHF Cardiology Director at The Ohio State University.
Kalki Bommaraju MD MPH
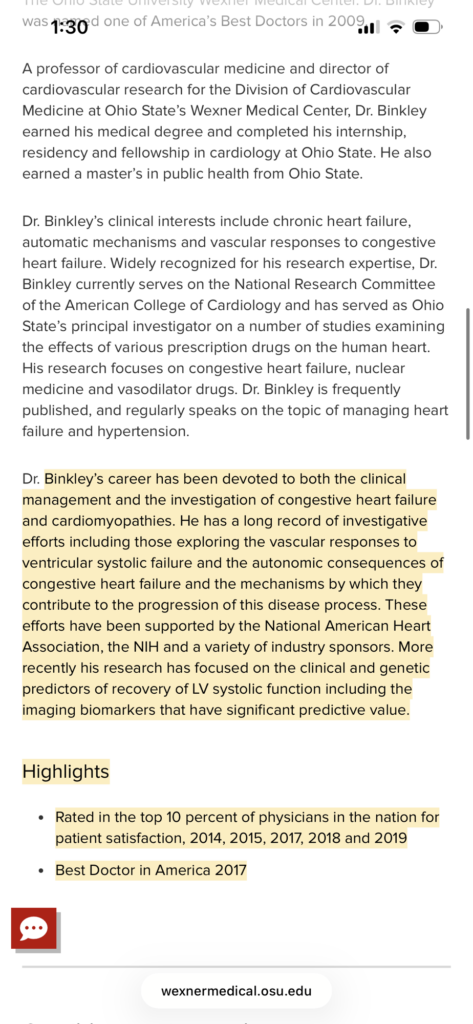
this is my research mentor:
Philip F Binkley MD MPH
THE OHIO STATE UNIVERSITY
imagine if NAD+ infusions of say 250ml weekly or monthly prevented CHF exacerbations by providing stunned or weakened myocardial and endocardial cells with extra NAD+. perhaps weekly infusions of NAD+ provide extra cellular power to help the cell’s metabolism to regenerate myocardium or endocardoum or purkinje fibers or neurons. the possibilties are endless and should all be studied given how cheap this medication is and how effective it has been shown to be in these preliminary studies. perhaps even ocular tissue could be helped to regenerate. basically my theory is that NAD+ infusions help the body heal and regenerate itself and therefore could be the key to living forever.
kalki bommaraju md mph
1:55 am
3/28/2026
paypal bobmarleyluveforever@gmail.com if you feel like u can donate some money to help fund this clinical trial of CURING ALL DISEASES FOR EVERYONE FOR BASICALLY NOTHING. $15 MAX PER MONTH ACTUAL COST FOR AN NAD+ IV INFUSION. ACTUAL COST.
The IV-medical.com NAD plus IV infusion CLINICAL TRIAL (FOUNTAIN OF YOUTH CLINICAL TRIAL)
At IV-medical.com we offer the NAD plus IV infusion as part of a thoughtful and medically grounded approach to supporting cellular energy metabolism and overall patient well being. NAD plus is a critical cofactor in human physiology that participates directly in glycolysis and the Krebs cycle by accepting electrons and forming NADH which then feeds into oxidative phosphorylation to ultimately drive the conversion of ADP to ATP. In theory increasing the availability of NAD plus may support these pathways and improve the efficiency of cellular energy production particularly in states where NAD plus levels may be relatively depleted such as aging metabolic stress or illness. Although the measurable biochemical benefit in otherwise healthy individuals is likely modest due to tight physiologic regulation and the fact that NAD plus is not usually the primary limiting factor in ATP generation we acknowledge that there is a growing body of anecdotal clinical experience suggesting that patients frequently report increased energy improved mental clarity and an overall sense of well being following NAD plus IV infusions. These subjective benefits while not yet strongly supported by large scale internal medicine randomized trials are meaningful to patients and are one of the reasons this therapy continues to be offered in carefully selected settings. At IV-medical.com we believe it is appropriate to provide therapies that may offer benefit when done responsibly and transparently while clearly communicating the limits of current evidence.
At the same time we emphasize that safety and proper medical practice are paramount. Any IV infusion including NAD plus requires appropriate clinical assessment prior to administration. This includes evaluation of the patient’s volume status comorbid conditions and most importantly basic laboratory values. Serum sodium must be checked prior to administration of IV fluids because administering intravenous fluids without knowing the sodium level can lead to serious complications including worsening hyponatremia or hypernatremia which can result in neurologic injury. Giving IV fluids without checking sodium is a deviation from standard medical practice and may constitute malpractice unless the patient is in an emergent hypotensive state where immediate fluid resuscitation is required. Therefore at IV-medical.com we strongly advocate that patients undergoing NAD plus IV infusion have appropriate laboratory evaluation including electrolytes prior to treatment unless there is a clear emergency indication. This ensures that we are not only offering a therapy that may provide symptomatic benefit but also adhering to the highest standards of internal medicine and patient safety.
In summary the IV-medical.com NAD plus IV infusion is based on a biologically plausible mechanism involving cellular energy metabolism and while its objective benefits may be modest in many individuals there is consistent anecdotal evidence of improved energy and well being in patients who receive it. We believe it is a reasonable therapy to offer within a medically supervised framework that prioritizes appropriate screening laboratory evaluation and adherence to safe infusion practices.
Selected Internal Medicine and Related Literature on NAD plus Biology and Metabolism
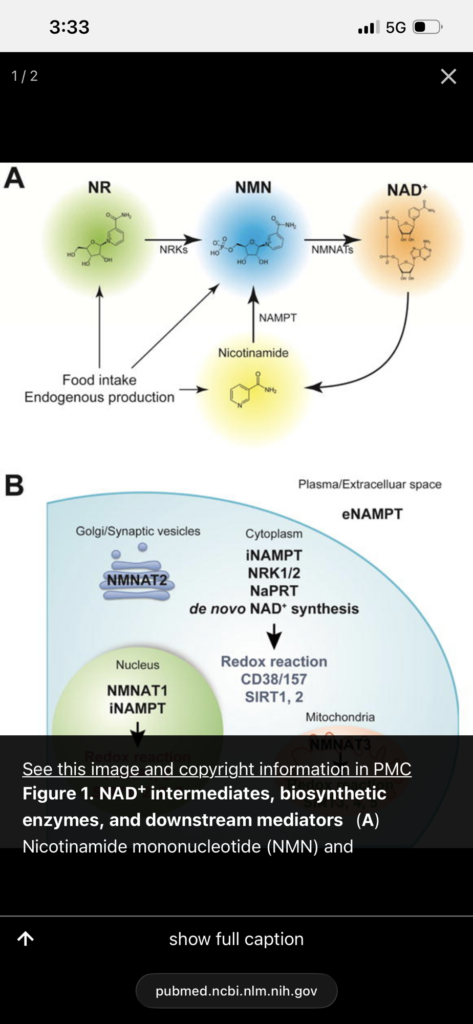
NAD Intermediates The Biology and Therapeutic Potential of NMN and NR
Yoshino J Baur J A Imai S I
Cell Metabolism
2018
NAD plus metabolism and its roles in cellular processes during ageing
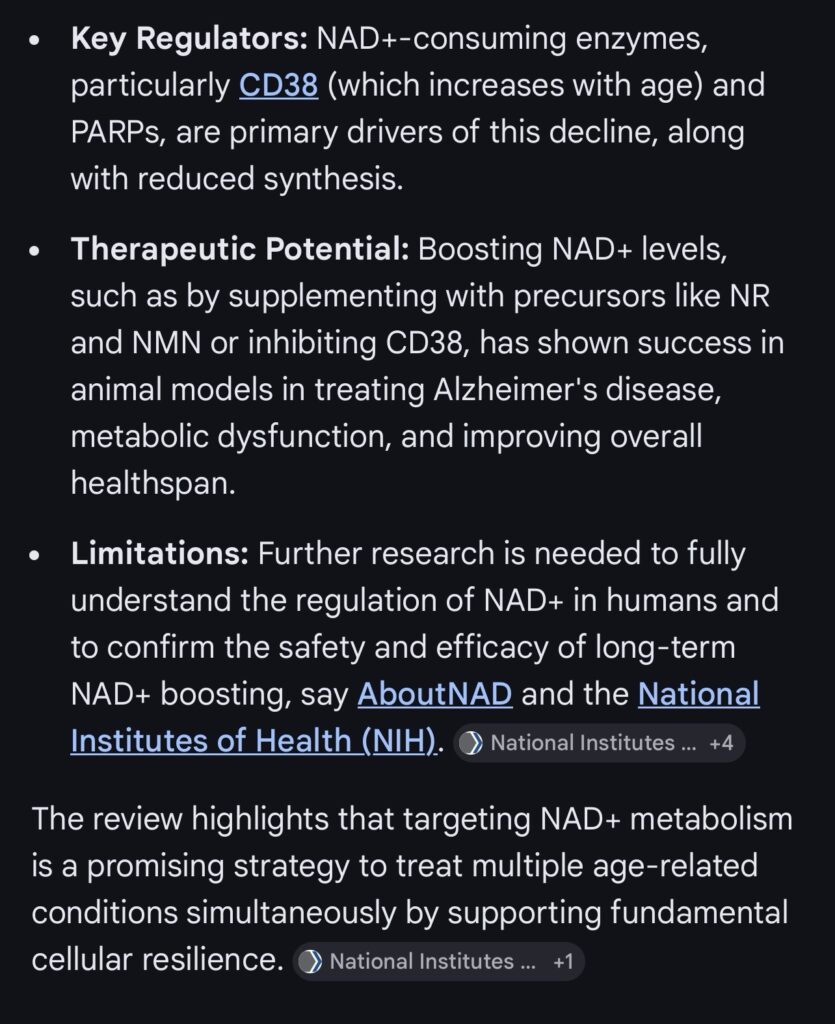
Covarrubias A J Perrone R Grozio A
Nature Reviews Molecular Cell Biology
2021
Role of NAD plus in regulating cellular and metabolic signaling pathways
Amjad S et al
Molecular Metabolism
2021
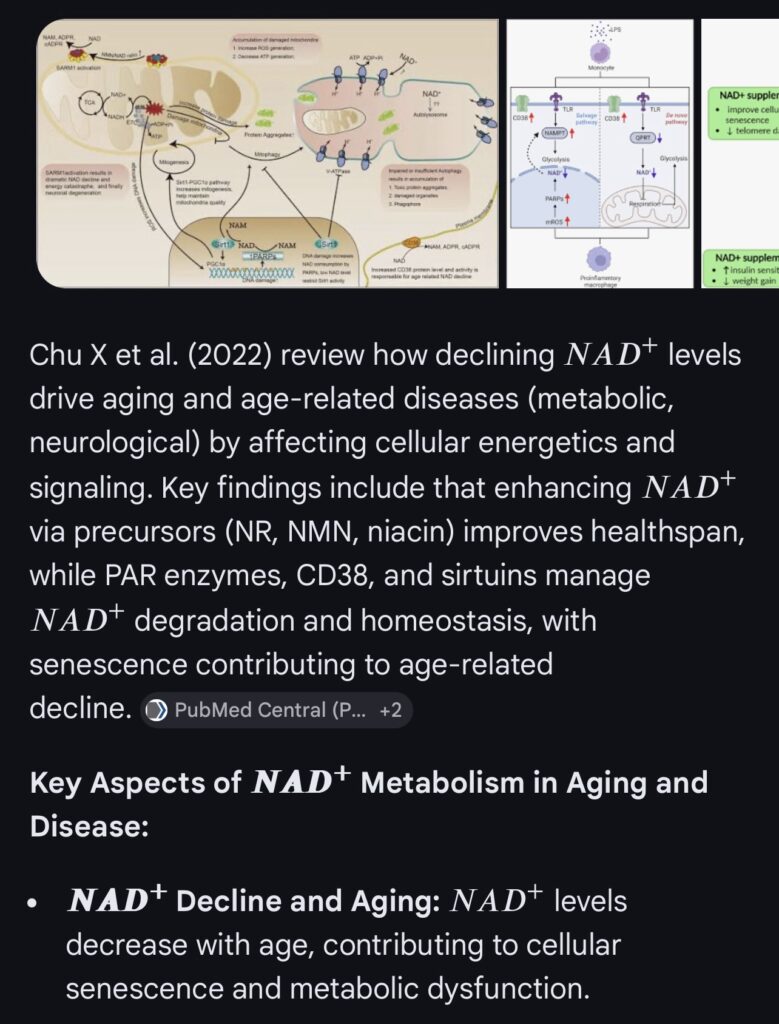
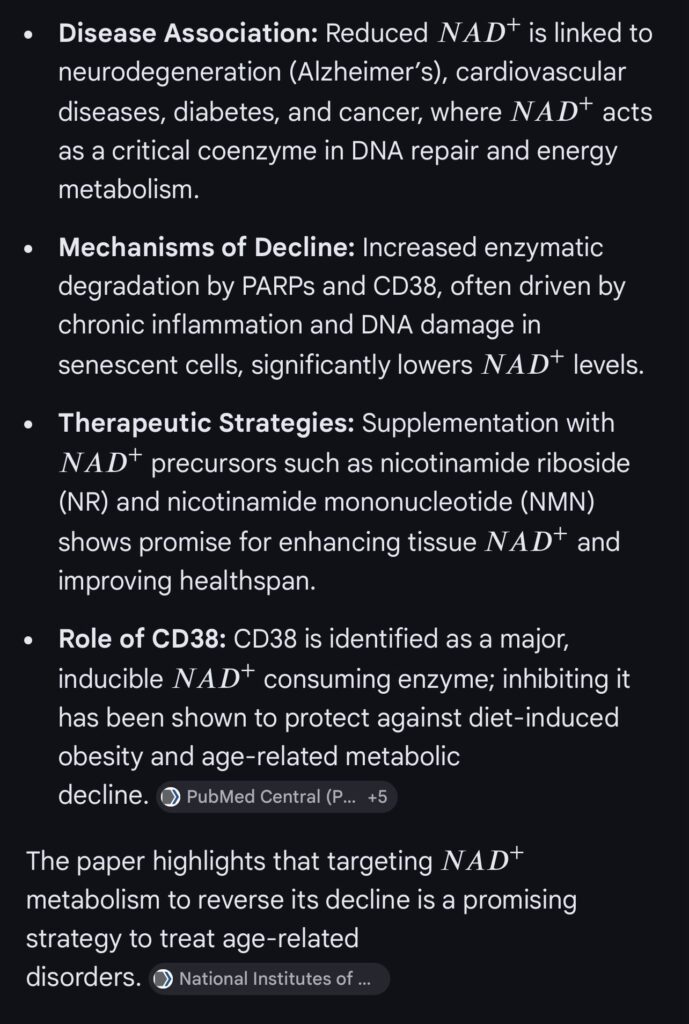
Regulation of NAD plus metabolism in aging and disease
Chu X et al
Metabolism
2022
FOUNTAIN OF YOUTH CLINICAL TRIAL
Frankly
Ohio
Understands
New
Truths
Always
In
News
Ohio
Finds
Youth
Over
Under
Tomorrow
Hospitals Suck so get NAD+ infusions that cure all your diseases, prevent you from aging, and make you live forever if you do it monthly.
that is my hypothesis.
lmk what u think Dr B
Kalki Bommaraju MD MPH
this is my research mentor:
Philip F Binkley MD MPH
THE OHIO STATE UNIVERSITY
imagine if NAD+ infusions of say 250ml weekly or monthly prevented CHF exacerbations by providing stunned or weakened myocardial and endocardial cells with extra NAD+. perhaps weekly infusions of NAD+ provide extra cellular power to help the cell’s metabolism to regenerate myocardium or endocardoum or purkinje fibers or neurons. the possibilties are endless and should all be studied given how cheap this medication is and how effective it has been shown to be in these preliminary studies. perhaps even ocular tissue could be helped to regenerate. basically my theory is that NAD+ infusions help the body heal and regenerate itself and therefore could be the key to living forever.
kalki bommaraju md mph
1:55 am
3/28/2026
paypal bobmarleyluveforever@gmail.com if you feel like u can donate some money to help fund this clinical trial of CURING ALL DISEASES FOR EVERYONE FOR BASICALLY NOTHING. $15 MAX PER MONTH ACTUAL COST FOR AN NAD+ IV INFUSION. ACTUAL COST.
NAD+ Augmentation to Improve Metabolic, Cardiac, and Neurocognitive Function: A Randomized Controlled Trial Across High-Risk Adult Cohorts
Principal Investigators
Tontania English RN – registered nurse
Kalki Bommaraju MD MPH – internal medicine doctor
Philip F Binkley MD MPH – cardiologist
Experience
Clinical management of patients with metabolic disease, heart failure, and complex chronic illness
Experience in inpatient and outpatient medicine
Interest in translational physiology and systems-level disease mechanisms
Personal Statement
Our clinical experience has emphasized the limitations of disease-specific treatment models and the need for therapies targeting shared underlying biologic mechanisms. This proposal represents a translational approach bridging NAD+ biology with clinical outcomes.
Project Summary / Abstract
Age-related decline in NAD+ is associated with mitochondrial dysfunction, impaired metabolic regulation, and reduced cellular resilience. Preclinical studies demonstrate that restoration of NAD+ improves metabolic, cardiac, and neurocognitive function. However, rigorous randomized controlled trials in humans remain limited.
This study proposes a multi-cohort, randomized, double-blind, placebo-controlled trial evaluating NAD+ augmentation in four high-risk populations: prediabetes, early dementia, heart failure, and obesity. Each cohort targets a clinically meaningful condition with validated endpoints while testing a shared mechanistic hypothesis that restoration of NAD+ improves mitochondrial and metabolic function across organ systems.
A total of 400 participants will be enrolled, with 100 participants in each cohort. Within each cohort, participants will be randomized 1:1 to receive NAD+ infusion or placebo for 6 months, with follow-up through 12 months. Primary outcomes are cohort-specific and include insulin sensitivity, cognitive performance, functional capacity, and body composition. Secondary outcomes include mitochondrial biomarkers, physiologic monitoring, and NAD+ levels.
This study will provide the first rigorous evaluation of NAD+ augmentation across multiple disease domains and determine whether targeting a core metabolic pathway yields clinically meaningful benefit.
Specific Aims
Overall Hypothesis
Restoration of NAD+ improves mitochondrial and metabolic function, leading to measurable improvements in disease-specific outcomes across multiple high-risk populations.
Aim 1
Determine whether NAD+ augmentation improves insulin sensitivity in adults with prediabetes.
Primary Outcome: Change in HOMA-IR and glucose tolerance.
HOMA-IR stands for Homeostatic Model Assessment of Insulin Resistance.
It is a method used to estimate how resistant a person is to insulin using fasting laboratory values.
What it measures
It estimates how much insulin the body needs to maintain normal blood glucose levels.
Higher insulin levels relative to glucose suggest insulin resistance.
Lower insulin levels with normal glucose suggest good insulin sensitivity.
Fasting insulin is measured in micro units per milliliter (µU/mL).
Fasting glucose is measured in milligrams per deciliter (mg/dL).
Example
If fasting glucose is 100 and fasting insulin is 10:
HOMA-IR = (10 × 100) / 405 = approximately 2.47
Interpretation (approximate ranges)
Around 1.0 indicates normal insulin sensitivity
1.5 to 2.0 suggests early insulin resistance
Greater than 2.5 suggests insulin resistance
Greater than 3.0 suggests significant insulin resistance
Ranges can vary depending on the population and laboratory standards.
Why it is used
HOMA-IR is commonly used in clinical studies because it is simple, inexpensive, and can be repeated over time to track changes in metabolic function.
Limitation
It is an estimate and not a direct measurement.
The gold standard for measuring insulin sensitivity is the hyperinsulinemic-euglycemic clamp, which is more complex and resource-intensive.
Aim 2
Determine whether NAD+ augmentation improves cognitive function in adults with early dementia.
Primary Outcome: Change in standardized cognitive scores (MoCA, ADAS-Cog).
MoCA stands for Montreal Cognitive Assessment.
It is a screening test used to detect mild cognitive impairment and early dementia.
What it measures
It evaluates multiple areas of cognition, including attention, memory, language, executive function, visuospatial ability, and orientation.
Structure
The test is scored out of 30 points and takes about 10 minutes to complete.
Interpretation
A score of 26 to 30 is considered normal
A score below 26 suggests cognitive impairment
Lower scores indicate greater impairment
Why it is used
MoCA is sensitive for detecting early cognitive decline and is commonly used in clinical studies because it can detect subtle changes over time.
ADAS-Cog stands for Alzheimer’s Disease Assessment Scale – Cognitive Subscale.
It is a more detailed cognitive test used primarily in Alzheimer’s disease research and clinical trials.
What it measures
It evaluates memory, language, attention, and other cognitive functions in more detail than screening tests.
Structure
The score typically ranges from 0 to 70 depending on the version used.
Interpretation
Lower scores indicate better cognitive function
Higher scores indicate worse cognitive function
An increase in score over time suggests worsening cognition
A decrease in score suggests improvement
Why it is used
ADAS-Cog is widely used in clinical trials because it is sensitive to changes in cognitive performance over time, especially in patients with established dementia.
Key difference
MoCA is a short screening tool used to detect early cognitive changes, and higher scores are better.
ADAS-Cog is a more detailed assessment used in research settings, and lower scores are better.
Why both are used in studies
Using both tests provides a more complete evaluation of cognition. MoCA helps detect early or subtle changes, while ADAS-Cog measures more detailed changes over time.
Aim 3
Determine whether NAD+ augmentation improves functional capacity in patients with heart failure.
Primary Outcome: Change in 6-minute walk distance and NT-proBNP.
Aim 4
Determine whether NAD+ augmentation improves metabolic health in adults with obesity.
Primary Outcome: Change in body composition (DEXA) and insulin sensitivity.
Secondary Aim
Evaluate changes in mitochondrial function, NAD+ levels, inflammatory markers, and physiologic stability across all cohorts.
Research Strategy
Significance
Chronic diseases including diabetes, dementia, heart failure, and obesity share upstream mechanisms involving mitochondrial dysfunction and impaired cellular energetics. Current therapies primarily target disease-specific pathways rather than underlying metabolic dysfunction.
NAD+ is a central regulator of mitochondrial function, DNA repair, and metabolic signaling. Declining NAD+ levels are associated with aging and multiple disease states. Restoration of NAD+ improves metabolic and functional outcomes in preclinical models, but clinical evidence in humans is limited.
This study addresses a critical gap by testing whether NAD+ augmentation produces clinically meaningful improvements across multiple disease domains using a rigorous randomized controlled design.
Innovation
This study is innovative because it targets a shared upstream metabolic pathway across multiple diseases rather than isolated downstream processes. It represents the first randomized controlled evaluation of intravenous NAD+ across multiple clinical populations. It integrates metabolic, cognitive, and functional endpoints into a unified design and incorporates continuous physiologic monitoring for exploratory biomarker discovery.
Approach
Study Design
Multi-cohort, randomized, double-blind, placebo-controlled trial with four parallel cohorts: prediabetes, early dementia, heart failure (NYHA class II–III), and obesity. Participants are randomized 1:1 within each cohort.
Sample Size
Total n = 400 participants
100 participants per cohort
50 NAD+ and 50 placebo per cohort
Sample size is powered to detect clinically meaningful differences in primary outcomes within each cohort.
Population
Inclusion Criteria
Age 40–70
Diagnosis specific to cohort (prediabetes, early dementia, heart failure, or obesity)
Ability to provide informed consent
Exclusion Criteria
Contraindications to infusion therapy
Intervention
Experimental Group
Intravenous NAD+ infusion administered weekly for 12 weeks followed by maintenance dosing per protocol
Control Group
Placebo infusion (normal saline) with identical administration schedule
Primary Outcomes
Prediabetes
Insulin sensitivity (HOMA-IR or hyperinsulinemic-euglycemic clamp)
Dementia
Cognitive performance (MoCA, ADAS-Cog)
Heart Failure
6-minute walk distance
NT-proBNP levels
Obesity
Body composition (DEXA)
Insulin sensitivity
Secondary Outcomes (All Cohorts)
NAD+ levels
Inflammatory markers
VO2 max
Resting energy expenditure
Quality of life measures
Exploratory Outcomes
Continuous glucose monitoring
Heart rate variability
Wearable device data
AI-based physiologic pattern analysis
Data Collection
Baseline
Metabolic laboratory testing
Functional testing
Body composition analysis
NAD+ level measurement
Follow-Up
Monthly laboratory monitoring
Functional testing at 3 and 6 months
Continuous wearable monitoring
Final assessment at 12 months
Statistical Analysis
Intention-to-treat analysis
Mixed-effects models for repeated measures
Between-group comparisons within each cohort
Secondary pooled analyses across cohorts
Adjustment for baseline covariates
Potential Problems and Alternative Strategies
If effect sizes are smaller than expected, sensitive endpoints and subgroup analyses will be used. If heterogeneity is observed across cohorts, analyses will remain cohort-specific with secondary pooled exploratory analysis.
Timeline
Year 1: Study setup and enrollment
Year 2: Intervention and data collection
Year 3: Data analysis and publication
Investigator Biosketch (Abbreviated)
Name: Tontania English, RN
Kalki Bommaraju MD MPH
Philip F Binkley MD MPH
Role: Principal Investigators
Training
Registered Nurse
Doctor of Medicine, Internal Medicine
Cardiologist
Experience
Clinical management of patients with metabolic disease, heart failure, and complex chronic illness
Experience in inpatient and outpatient medicine
Interest in translational physiology and systems-level disease mechanisms
Personal Statement
Our clinical experience has emphasized the limitations of disease-specific treatment models and the need for therapies targeting shared underlying biologic mechanisms. This proposal represents a translational approach bridging NAD+ biology with clinical outcomes.
Budget (Estimated, 3-Year Project)
Total estimated budget: 3.0 to 3.8 million USD
Major cost categories include personnel, infusion services, laboratory assays, imaging (DEXA), cognitive testing, wearable monitoring devices, and data management systems.
Overall Impact
This study directly tests whether restoring NAD+ levels can modify fundamental metabolic and physiologic processes across multiple disease states. Positive findings would support a new therapeutic framework targeting shared mechanisms of aging and chronic disease and justify larger multicenter trials.
Significance (Additional Rationale: Real-World Use and Evidence Gap)
NAD+ intravenous infusion therapy is increasingly being offered through a rapidly expanding number of outpatient infusion centers across the United States. These services are being marketed directly to consumers with claims related to improved energy, cognitive function, metabolic health, and aging-related outcomes. Despite widespread adoption, there is a lack of rigorous clinical trial data evaluating the safety, efficacy, optimal dosing, and appropriate patient selection for this intervention.
As a result, a growing number of patients are receiving NAD+ infusions in real-world settings without an established evidence base to guide clinical decision-making. This creates a critical gap between clinical practice and scientific validation. In the absence of controlled studies, clinicians, patients, and regulatory bodies lack reliable data regarding therapeutic benefit, potential risks, and long-term outcomes.
The widespread, unsupervised use of NAD+ infusion therapy underscores the urgency of conducting a well-designed randomized controlled trial. Such a study is necessary not only to evaluate efficacy, but also to define safety profiles, identify populations most likely to benefit, and establish standardized protocols for administration and monitoring.
This proposal directly addresses this gap by providing a rigorous, controlled evaluation of NAD+ augmentation across multiple clinically relevant populations. Given the current scale of real-world use, generating high-quality evidence is essential to inform clinical practice, guide patient care, and support evidence-based policy decisions.
First controlled trial evaluating IV NAD⁺ in humans Direct translation of NAD⁺ biology into clinical intervention Integration of physiologic and metabolic endpoints
Significance
This study directly tests whether restoring NAD⁺ levels can modify metabolic dysfunction in humans, addressing a central mechanism implicated in aging and chronic disease.
Future Directions
If successful, this study will support:
Larger multicenter trials Extension into cardiovascular, neurologic, and aging populations Development of NAD⁺-targeted therapies
NAD⁺ Restoration and the Future of Aging: What the Science Suggests Over the Next 20 Years
Over the past decade, a growing body of research has converged on a central idea in aging biology: declining levels of NAD⁺ (nicotinamide adenine dinucleotide) are not just a byproduct of aging, but a driver of it.
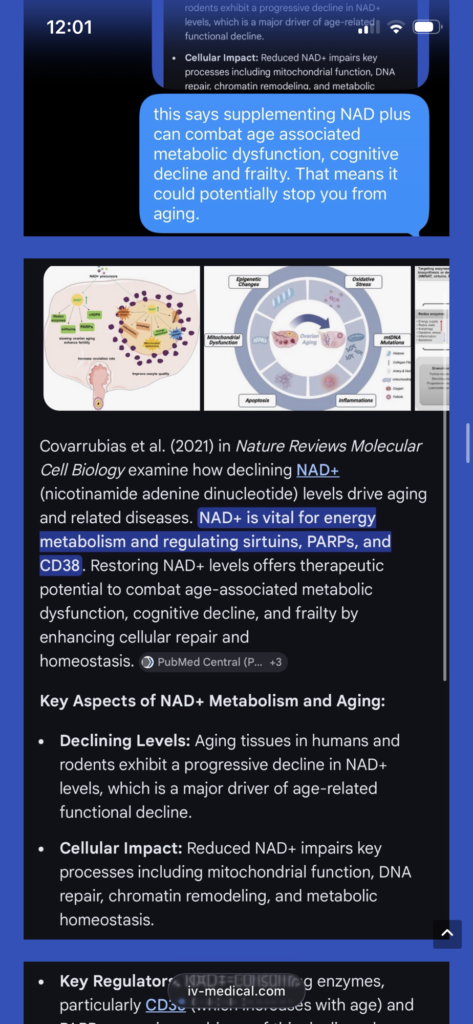
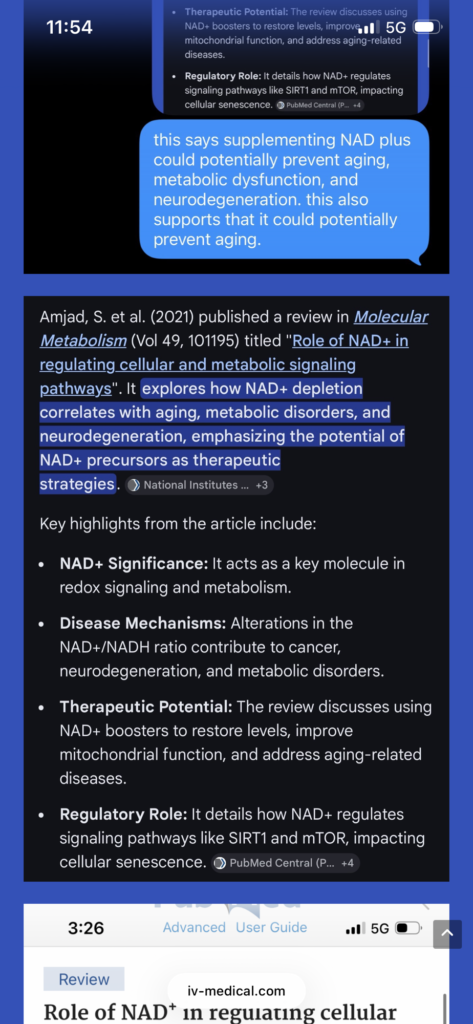
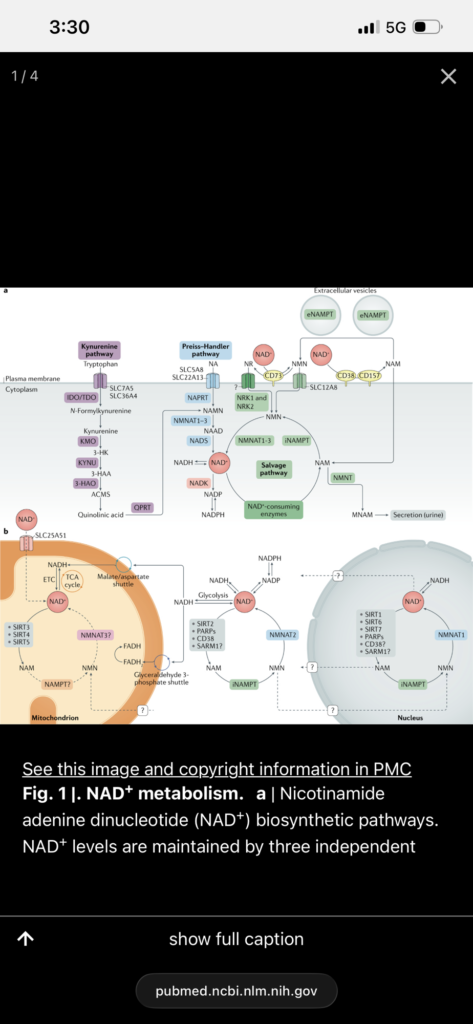
Key review papers—including Yoshino et al. (2018), Covarrubias et al. (2021), Amjad et al. (2021), and Chu et al. (2022)—all point to the same underlying mechanism. NAD⁺ is essential for mitochondrial function, DNA repair, and regulation of critical signaling pathways such as sirtuins, PARPs, and CD38. As NAD⁺ levels fall with age, these systems become progressively impaired, contributing to metabolic disease, reduced cellular resilience, and functional decline.
What makes this pathway particularly compelling is that it is modifiable.
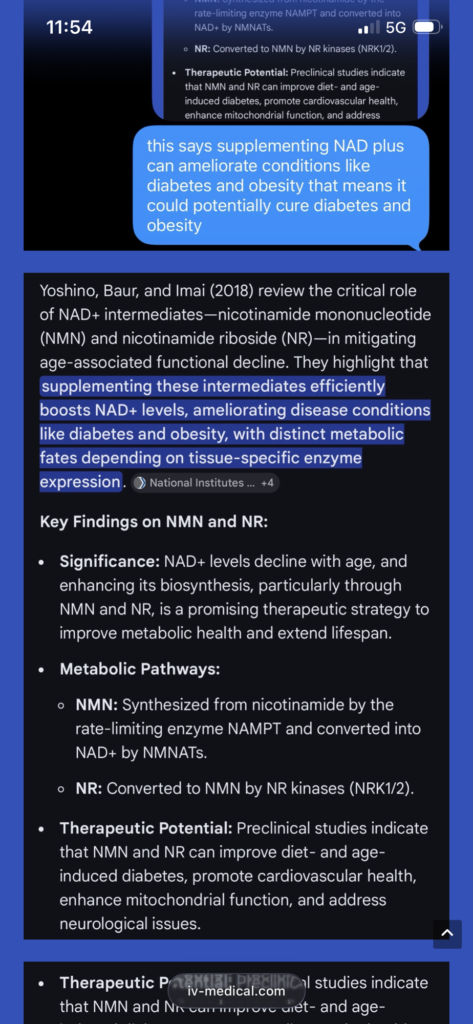
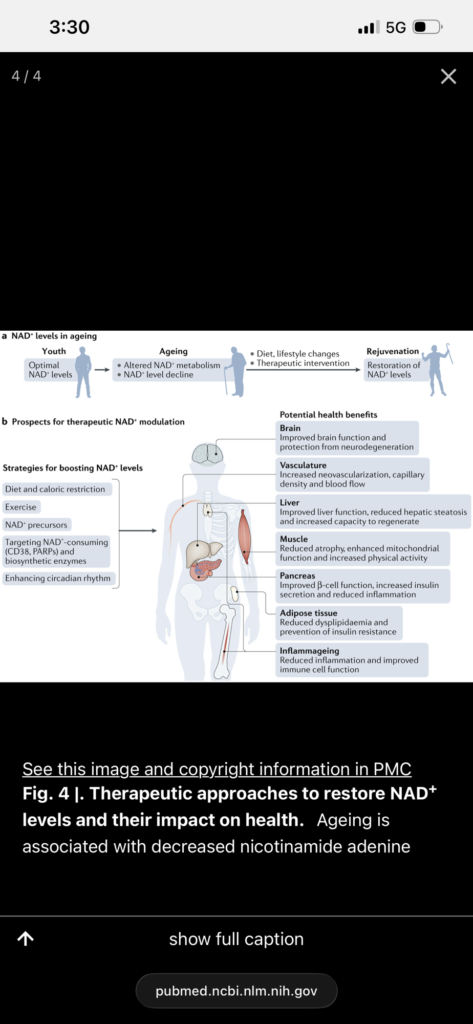
Supplementation with NAD⁺ precursors such as nicotinamide mononucleotide (NMN) and nicotinamide riboside (NR) has been consistently shown to restore NAD⁺ levels. In preclinical models, this restoration produces widespread effects: improved mitochondrial function, enhanced metabolic efficiency, reversal of insulin resistance, and protection against diet-induced obesity. These changes are not isolated—they reflect a shift in cellular biology toward a more youthful functional state.
Human studies have already confirmed that NAD⁺ levels can be reliably increased with supplementation. Early clinical data suggests improvements in metabolic markers and functional outcomes, though long-term endpoints are still being studied.
The key question is not whether NAD⁺ can be restored—it can. The question is what happens when it is maintained over decades.
If the mechanisms observed in preclinical models continue to translate into human physiology, the long-term implications are significant. Sustained NAD⁺ repletion would be expected to preserve mitochondrial function, maintain more efficient cellular energy production, and support ongoing DNA repair. Over time, this could reduce the cumulative burden of cellular damage that drives aging-related decline.
From a metabolic standpoint, maintaining higher NAD⁺ levels may blunt the progression of insulin resistance, reduce the likelihood of obesity-related dysfunction, and stabilize energy homeostasis. From a neurological perspective, improved cellular maintenance and reduced inflammatory signaling could help preserve cognitive function. At the systemic level, this translates into a slower trajectory of age-associated disease.
Looking 20 years ahead, the expected outcome is not the elimination of aging, but a meaningful alteration of how it presents.
Individuals maintaining optimized NAD⁺ levels over long periods would be expected to retain higher levels of physical function, metabolic stability, and cellular resilience compared to typical aging populations. Rather than the standard progression toward frailty, metabolic disease, and cognitive decline, the trajectory may shift toward prolonged functional independence and delayed onset of age-related conditions.
In this sense, NAD⁺ restoration represents a shift in strategy—from treating individual diseases to targeting the underlying biology that connects them.
The science is still evolving, and long-term human data will ultimately define the magnitude of these effects. However, the consistency across mechanistic studies, animal models, and early human trials suggests that NAD⁺ biology is not a fringe concept—it is a central regulator of how we age.
If that holds true, the next 20 years may not eliminate aging—but they may significantly redefine it.
Prospective, Open-Label, Longitudinal Cohort Study Evaluating the Clinical, Functional, and Biomarker Effects of Intravenous NAD⁺ Infusion With Continuous Digital Monitoring Over 20 Years i.e. FOUNTAINOFYOUTH CLINICAL TRIAL
Frankly Ohio Understands New Truths Always In News Ohio Finds Youth Over Under Tomorrow
Frankly Ohio Understands New Truths Always In News Ohio Finds Youth Over Under Tomorrow
Study Design
Prospective, open-label, non-randomized cohort study with no blinding. Both the patient and the physician know the patient is receiving NAD⁺ infusion therapy. Patients are followed for 20 years with structured assessments every 6 months and continuous digital monitoring.
Objectives
Primary Objective
To evaluate whether long-term NAD⁺ infusion therapy is associated with disease progression, disease regression, hospitalization rates, and survival across a broad real-world patient population.
Secondary Objectives
To evaluate changes in functional status, quality of life, physiologic aging markers, video-based appearance and movement over time, continuously collected home vital sign data, laboratory trends, and disease-specific biomarkers including BNP in CHF patients.
Population
Inclusion Criteria
Adults age 18 years or older
Willing to receive NAD⁺ infusions
Willing to participate in longitudinal follow-up
Willing to allow clinical data, video data, home monitoring data, and laboratory data to be stored in the study database and analyzed by AI
Exclusion Criteria
None
Patients with all levels of illness severity may be enrolled, including stage IV cancer, congestive heart failure, neurodegenerative disease, advanced frailty, and multiple chronic medical conditions.
Intervention
Patients receive intravenous NAD⁺ infusion according to the treating physician’s clinical protocol. Dose, frequency, infusion duration, and treatment changes are documented in the medical record and study database.
Specialty-Directed NAD⁺ Infusion Determination
For all enrolled patients, NAD⁺ infusion parameters including dose, volume, rate, and frequency are determined based on the patient’s underlying medical conditions, with oversight by the appropriate physician as outlined below.
Oncology
For patients with active or prior malignancy, NAD⁺ infusion parameters are determined by an oncologist.
Hematology
For patients with hematologic conditions, NAD⁺ infusion parameters are determined by a hematologist.
Neurology
For patients with neurologic conditions, NAD⁺ infusion parameters are determined by a neurologist.
Pulmonary Medicine
For patients with pulmonary conditions, NAD⁺ infusion parameters are determined by an internal medicine physician or hospitalist.
Critical Care
For patients with critical illness or conditions requiring intensive monitoring, NAD⁺ infusion parameters are determined by an internal medicine physician or hospitalist.
Gastrointestinal Conditions
For patients with gastrointestinal disorders, NAD⁺ infusion parameters are determined by an internal medicine physician or hospitalist.
Other Internal Medicine Conditions
For all other conditions falling within internal medicine, NAD⁺ infusion parameters are determined by an internal medicine physician or hospitalist.
Non–Internal Medicine Conditions
For any medical condition outside traditional internal medicine specialties, NAD⁺ infusion parameters are determined by an internal medicine physician or hospitalist only.
Disease-Specific Treatment Modifications
Congestive Heart Failure
Patients with congestive heart failure receive reduced-volume or slower-rate NAD⁺ infusions based on tolerance. Lower volumes such as approximately 250 mL or less may be used. Infusion parameters are determined and adjusted by a cardiologist. Clinical decision-making may consider volume status, ejection fraction, symptoms, blood pressure, heart rate, recent hospitalizations, and BNP trends.
Chronic Kidney Disease and End-Stage Renal Disease
Patients with chronic kidney disease or end-stage renal disease receive individualized NAD⁺ infusion protocols. Volume, concentration, and rate are determined based on renal function, volume status, dialysis status, and electrolyte balance. Infusion parameters are determined and adjusted by a nephrologist. For patients on dialysis, infusion timing may be coordinated with dialysis sessions and adjusted to avoid fluid overload.
Follow-Up Schedule
Patients are followed for 20 years.
Every 6 Months
At each 6-month interval, the following are documented:
new diagnoses
disease progression
disease regression
hospitalizations
medication changes
changes in symptoms
functional status
quality of life
physician assessment
A video of the patient is recorded at each assessment to document facial appearance, skin appearance, posture, gait, movement, speech, and general visible aging characteristics.
Home Monitoring
Home data may include blood pressure, body weight, heart rate, home ECG monitoring, and future home laboratory testing using fingerprint or micro-blood collection technology when available. All home data are uploaded automatically into the study database when technically available.
Patients may also be provided with a home cardiac monitoring system. If a device exists with monitoring and built-in defibrillation capability suitable for outpatient use, that device may be used as part of the monitoring system.
CHF Subgroup Monitoring
Patients with congestive heart failure may undergo serial or continuous BNP monitoring to determine whether BNP predicts increased hospitalization risk. BNP levels are correlated with symptoms, hospitalizations, and clinical deterioration.
Data Collection
The following are stored in the database:
infusion records
physician notes
diagnoses
disease progression or regression assessments
laboratory values
vital signs
home monitoring data
video recordings
hospitalization data
survival data
AI Analysis
The database is continuously analyzed by AI for trend detection, disease progression patterns, disease regression patterns, aging progression or regression patterns, prediction of clinical deterioration, abnormal vital sign detection, abnormal laboratory detection, and cardiac risk detection.
If an abnormality is detected, the physician is notified.
Endpoints
Primary Endpoints
disease progression over time
disease regression over time
all-cause hospitalization
disease-specific hospitalization
all-cause mortality
Secondary Endpoints
change in blood pressure
change in weight
change in heart rate
change in laboratory markers
change in BNP in CHF patients
AI-derived risk scores
visual and functional aging trajectory over time
Safety Monitoring
Adverse events are recorded continuously. Infusion-related complications are tracked. AI-triggered alerts are reviewed by the physician. Periodic safety review is performed annually.
Study Nature
This is an open-label observational cohort study designed to follow all patients receiving NAD⁺ therapy in a real-world setting, including patients with severe and advanced disease, to determine whether measurable benefit, no effect, or harm is observed over long-term follow-up.
I have outlined three FCA cases that I have sent to multiple law firms. They have all declined to take these cases. I am therefore reaching out directly because I believe this requires federal attention.
I believe that you and President Donald Trump have what it takes to address these issues and help fix systemic problems in our medical system. I am willing to do whatever is necessary to assist.
I want to be transparent about my background. My first girlfriend’s father, Stephen Donohoe, is best friends with President Joe Biden, and I did vote for President Biden. Sidenote it really is true. At the same time, I also love President Trump, and I was a HUGE fan of The Apprentice when it aired. I mention this because I believe the issues raised here cross all political lines. This is not political. This is about protecting the United States, its healthcare system, and taxpayers.
What I am describing involves medical corporations taking advantage of CMS, Medicare, Medicaid, and the American public. This is a systemic issue that affects everyone.
I am particularly concerned that my alma mater, The Ohio State University, may be involved in practices where patients are routed through the James Cancer Hospital to justify oncological billing even when there is no cancer diagnosis. I was told this by two physicians, including REDACTED, MD, and Dr. Sen Siva, who is a chief medical officer. Both are based in Columbus, Ohio. I believe this warrants investigation.
Throughout my career, I have always prioritized patient care. I examine my patients thoroughly and treat all individuals equally regardless of race, background, or circumstances. I trained at The Ohio State University, completed residency at Riverside Methodist Hospital, and have served as an attending physician at institutions including the University of Chicago, Midwestern University, and Loyola University. I have always held myself to a high standard.
What I have observed in practice has been deeply concerning. These issues have been present since my training, but as an attending physician, I have now experienced direct consequences for raising concerns.
I have also observed potential disparities in pain management. At Select Specialty Hospitals, I observed situations where white patients were receiving IV pain medications such as Dilaudid while Black patients were not. When I added appropriate pain control for Black patients, those medications were later removed by other physicians when I was off service, and patients and families continued to report uncontrolled pain. This pattern is concerning and should be reviewed.
I am requesting that these matters be investigated. I am willing to provide testimony, documentation, and any supporting materials needed.
Sincerely,
Dr. Kalki Bommaraju, MD, MPH
ADDITIONAL STATEMENT
My concern is that the system may have become so corrupt that even private attorneys are unwilling to pursue clear cases of medical fraud. I do not understand why multiple law firms would decline matters of this magnitude unless there are external pressures or systemic influences, such as healthcare industry lobbying, that discourage these cases from being brought forward. I believe this issue itself warrants investigation.
I am also concerned that physicians are effectively intimidated into complying with improper practices. When applying for credentialing at new hospitals, physicians must rely on prior institutions for references and approvals. If a physician raises concerns or reports misconduct, prior employers can negatively impact credentialing, making it difficult or impossible to continue practicing. This creates a system where doctors are discouraged from speaking out.
After being terminated by MedOne Healthcare Partners after approximately three months for raising concerns about what I believed to be clear fraud and other unclear reasons, I felt obligated to take action and report these issues.
I also want to clarify my background. I was a salutatorian in high school, a National Merit Scholar, and received a full scholarship for undergraduate education with guaranteed admission into medical school. I later obtained a Master of Public Health through an NIH-supported program. I have trained and practiced at multiple institutions and have always maintained high standards in patient care.
I believe that when these institutions are contacted, there may be attempts to discredit me. I want to make clear that I am a highly trained and experienced physician raising concerns in good faith.
Finally, I respectfully request that these concerns be shared with appropriate federal leadership. If possible, I would appreciate that President Donald Trump personally be made aware of these matters, as I would welcome the opportunity to discuss these issues in person.
ADDITIONAL STATEMENT
I would also like to provide additional context regarding disparities in pain management that I have observed over the course of my training and practice.
During my medical training at The Ohio State University Medical Center and Riverside Methodist Hospital between 2003 and 2011, patients with sickle cell disease were consistently scrutinized regarding their requests for pain medication. They were frequently characterized as drug-seeking, and this perspective was emphasized by instructors during training.
When I later practiced as an attending physician in Chicago, my experience was markedly different. Sickle cell patients were treated with a higher level of trust regarding their pain. When a patient stated that a specific dose of medication such as 2 milligrams or 3 milligrams of Dilaudid every 3 hours was required to control their pain, that information was generally respected and incorporated into treatment plans unless it was clearly unsafe.
In contrast, in Ohio, I observed that sickle cell patients were routinely prescribed significantly lower doses, such as 0.5 milligrams or 1 milligram of Dilaudid every 3 hours, regardless of what the patient reported as necessary for adequate pain control. This pattern appeared consistent and did not seem to be individualized based on patient needs.
Given that sickle cell disease disproportionately affects Black patients, I am concerned that this may reflect a broader pattern of unequal treatment. I believe this issue warrants careful review to determine whether there are systemic disparities in pain management practices affecting specific patient populations.
I respectfully request that these concerns be evaluated as part of a broader review of patient care practices perhaps even jointly by the DOJ and ACLU.
Finally, I believe that if Donald Trump addresses this problem, many people would respect him for defending the interests of Black patients.
Sorry for so many messages.
ADDITIONAL STATEMENT
I also want to add important context regarding why the racial disparities I observed in Ohio are especially concerning to me.
The first place in Ohio that I lived after leaving the Chicagoland area, where I lived from ages 5 through 10, was Middletown, Ohio. I attended Vail Middle School there, which was an all-Black middle school, and I lived in a townhouse community that was mostly Black residents. Before that, I lived in a townhouse community in Grand Island, New York, near Niagara Falls, where most of the residents were minorities, and my next-door neighbor was Black. In Chicago, I worked primarily on the South Side for many years, and most of my patients were Black.
Because of that background, when I observed at Select Specialty Hospital in Victorian Village in Columbus, Ohio, that Black patients were not being given IV Dilaudid while white patients were, it was deeply disturbing to me. I observed specific patients where I added IV Dilaudid for Black patients because their pain was not being adequately treated. When I later went off service, those medications would be removed by other physicians, and the patients and family members would continue to complain about uncontrolled pain.
I believe this may represent a violation of the civil rights of Black patients in Ohio who are admitted to these facilities. I believe this issue should be investigated by appropriate authorities, including the Attorney General of the United States, because I have specific patients on whom this occurred at Select Specialty Hospital in Victorian Village in Columbus, Ohio.
I also mention Middletown, Ohio, because I would like these concerns to be brought to the attention of Vice President J.D. Vance. He is from Middletown, and so am I. We both also attended The Ohio State University. I believe he would be deeply concerned by what I was told in Columbus, Ohio, regarding The Ohio State University Medical Center.
Specifically, I was told by physicians in Columbus that Ohio State was routing patients through the James Cancer Hospital in ways that justified or facilitated oncological billing for patients who did not actually have cancer or an oncological condition. I was told that patients might be passed through the James Cancer Hospital, have notes or services associated with that facility, and then be transferred elsewhere, creating a billing advantage or reducing the likelihood of denial. I believe this practice should be thoroughly investigated.
I respectfully request that these concerns regarding Columbus, Ohio, Select Specialty Hospital, and The Ohio State University Medical Center be reviewed carefully and shared with appropriate federal leadership.
Sincerely,
Kalki Bommaraju MD MPH
3/27/2026
electronically signed
contact kalkidoc@gmail.com if u feel like u want to help
are you a doctor? Do you have a blog or website when you can share all your thoughts and ideas about things going on in the medical community? If not, I’m looking for authors for this site. Please email me at kalkidoc@gmail.com if you’re interested in being an author.